Your patients quit in the first month. Brevva is why they don't.
A between-visit food-support layer for your GLP-1 patients' first 30 days — branded to your clinic, with everything medical sent straight back to your team.


Every patient is now harder to keep — and more expensive to replace.
Cheap compounded supply is gone. Patients face branded prices or narrower options, and the ones who drop in week three cost more to replace than they did a year ago.

One-year discontinuation among non-diabetic adults with obesity (JAMA Network Open / Prime Therapeutics, 2024–25). Early nausea per published GLP-1 trial data. Directional market context, not clinical guidance.
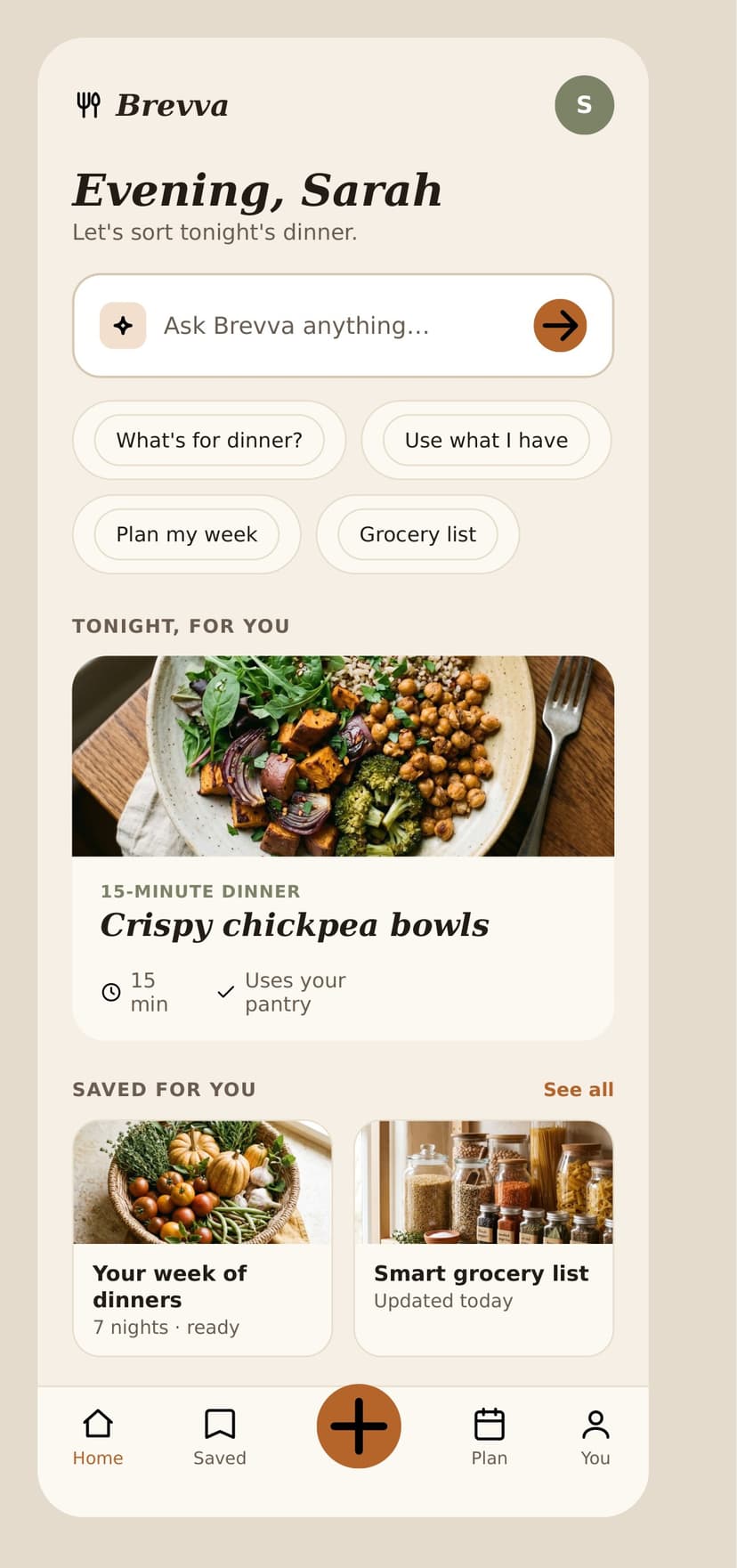
The daily food and side-effect questions — handled.
Brevva covers the between-visit questions that flood your inbox: what to eat, and how to eat through the side effects that make patients quit. All food guidance, every medical question routed back to you.
What do I even eat now?
Protein on a low appetite, small-meal structure, hydration, grocery lists, and simple meal ideas — every day of the first 30.
How do I eat through the nausea?
Nausea, constipation, low energy, early fullness, reflux — met with eating strategies: what to eat, when, and how much to ease it.
How do I make this stick?
Eating out, busy days, hydration reminders, and keeping the right staples on hand so a hard week doesn't end the program.

In three columns
Helps your patients with
- Small-meal structure
- Protein & hydration
- Nausea-friendly eating
- Grocery & planning help
Escalates back to you
- Symptoms & side effects
- Dose questions
- Anything medical
Never does
- Dosing or diagnosis
- Start / stop / switch
- Medication or effectiveness claims
A calm home for the questions that hit at 9pm.
Patients open Brevva on their phone — dinner ideas, nausea-friendly options, grocery help, and week planning. Food guidance only; anything clinical routes back to your team.
- Ask-anything food support between visits
- Tonight's dinner and weekly meal planning
- Pantry-aware suggestions — no patient data from you
Your patients sign up themselves. You never send us their data.
Brevva is a tool you refer patients to — not a service that holds your patients' records. Three steps, zero data exchange.
1 · Your clinic shares a QR
We give you a clinic-specific code and link. Your front desk hands it to the patient at the post-consult handoff.
2 · The patient signs up
They scan and create their own private account. Nothing comes from you — the patient enrolls directly.
3 · They get First 30
Daily food support through the first month, branded to your clinic, with anything medical routed back to your team.


One patient you keep pays for a year of this.
Prove it on your own patients in 30 days.
A free pilot designed to produce one number: how many of your patients are still on program at day 30.
See what your patients are really struggling with.
Fifteen minutes to walk the pilot — your QR, 30 days, a day-30 retention number against your baseline. No integration, no staff time.
Book a partner demoNutrition education only.Brevva provides food and nutrition support; it is not medical advice and not a substitute for a clinician. Medication, dosing, and symptom questions are escalated to the patient's clinic. Patients enroll directly; Brevva does not receive patient data from clinics.